
The objective of “Minimally Invasive Decompression for Lumbar Spinal Stenosis: The Impact of Moving to mild® Directly or After Initial ESI Failure on Clinical Performance—A Six Center Retrospective Report” was to understand how epidural steroid injection (ESI) use prior to mild® impacts patient outcomes. In this clinical study, 145 patients were divided into 2 groups receiving either 0-1 or 2+ ESI procedures prior to mild®. View the abstract poster below to discover the results of the retrospective report and learn why moving to mild® after the first ESI fails can put more spinal stenosis patients on the path to long-term relief.
Watch Dr. Peter Pryzbylkowski present his abstract from the American Society of Pain and Neuroscience’s (ASPN) Third Annual Conference in which he reviews the data and shares why he moves his lumbar spinal stenosis (LSS) patients to mild® earlier in the treatment journey.
Do you want to learn more about mild® and challenge your thinking around ESIs? Contact Vertos Medical for more information about the minimally invasive mild® Procedure and read about Dr. Jason Pope’s experience dealing with “Epidural Exhaustion” in his new blog.
Peter Pryzbylkowski, MD (00:00)
My name is Dr. Peter Pryzbylkowski. I’m a board certified anesthesiologist and board certified interventional pain specialist with the Relievus Pain Management Group, based out of the Philadelphia area. I want to thank Vertos, number one, for getting me involved with this study.
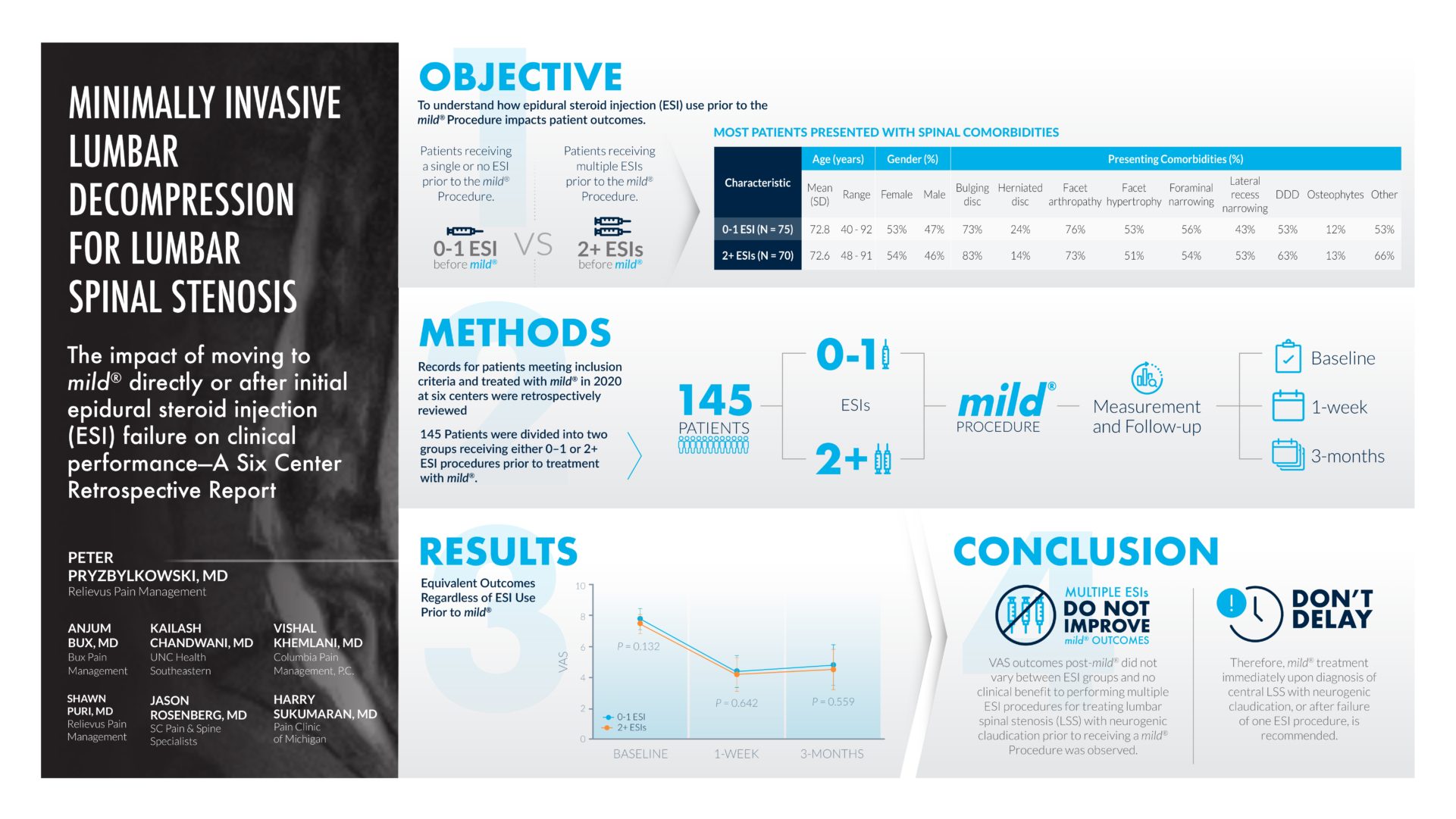
So, the objective of this study was to determine whether or not, no epidurals, one epidural versus a series of epidurals, made any difference in terms of pain relief, pain reduction, post-mild® Procedure. So, this is a nice clinical study because it kind of expands the bandwidth of practices across the country.
So, we have 6 total centers, 145 patients, that was enrolled in this study. Basically it was a retrospective review of patient charts we all did, and it’s important to notice, specifically under the objective tab, that the comorbid conditions coexisting, with patients with lumbar spinal stenosis with neurogenic claudication, is noted there, so these patients had bulging discs, herniated discs, facet arthropathy, facet hypertrophy, narrowing of the foramen, degenerative disc disease, osteophytes, and other comorbid conditions, so even though these patients had other comorbid conditions that are listed there, these patients still had good clinical and durable clinical results after post decompression procedure.
So, you can see the average ages there, the breakdown of male versus female, and those comorbid conditions I had mentioned before. And the groups we’re looking at, so it’s a group of patients who either had no epidurals or one epidural, versus two or more epidurals. So 145 patients total, were looked at in this retrospective review, and we followed the results, both at the baseline pre-procedure, one week post-operatively, and 3 months after mild® Procedure was performed. And, what you can see in the results section is that multiple epidurals versus no epidurals or one epidural did not make a difference in terms of VAS scores post-mild® Procedure.
(02:13) So, really what this is telling us as pain providers, is it doesn’t matter if you do no epidurals, one epidural or multiple. It’s not gonna affect your clinical outcome post-mild® Procedure, so the take home message from a retrospective review like this is that really, doing epidurals, a series of epidurals, really, we know as pain doctors, doesn’t really provide long-term clinical benefit, and it’s not gonna affect the outcome post-lumbar decompression. So if you have a patient with lumbar spinal stenosis with neurogenic claudication, they have ligamentum flavum hypertrophy, they’re candidates for the mild® Procedure and it’s important to do the procedure sooner rather than later ’cause all you’re really doing with a series of epidurals is delaying appropriate care, so kind of the message that this has hit home in my own personal practice is, I’ve really been able to go to all my advanced providers and say, “Listen, if we have patients who are kind of stuck in this rut of doing multiple epidurals, epidural, epidural, epidural for their lumbar spinal stenosis, we should really be considering doing the mild® Procedure to help give them good long-term benefit, rather than giving them multiple injections, which increases the risk of infection, increases the risk of an untoward side-effect.” Obviously every time we do a procedure there’s always a risk.
It’s nice to do a procedure that can give them long-term benefit, so if you have patients that have spinal stenosis, it’s just important to keep in mind mild® as a first treatment step rather than treatment that you would consider down the road for patients with spinal stenosis with neurogenic claudication. So I would not delay treating these patients when they come to my clinic. So, I used to do an epidural, 2 epidurals, 3 epidurals, for patients with spinal stenosis with neurogenic claudication. The outcomes really were hit or miss, so for me personally, I’m offering these patients percutaneous decompression in the form of the mild® Procedure a lot sooner than I used to 2-3 years ago. And the data from this retrospective study kind of shows that by doing the procedure sooner rather than later, not delaying care, we can give them good long-term benefit, give them a procedure that’s actually indicated for their pathology and approved for their pathology, rather than delaying care with a series of epidurals.
The following study, “Single-Center Comparison of Streamlined Technique Safety for mild® Procedure: Measuring Incidence of Postoperative Complications Compared to Standard Approach,” evaluates the safety of the Streamlined Technique in patients treated consecutively by a single center. As the mild® Procedure has become more widespread in clinical practice, there has been an evolution from the Standard Approach to the Streamlined Technique, a less invasive procedural approach. Dr. Navdeep Jassal and Christine Christensen, MSN, APRN, of the Spine & Pain Institute of Florida, evaluated 78 mild® patients treated using either the Streamlined Technique or the Standard Approach and measured the occurrence of postoperative complications. View the abstract poster below to discover the results of this study, and learn why the mild® Procedure should be considered the first-line intervention for patients with lumbar spinal stenosis after conservative treatments have been exhausted.
Watch Dr. Jassal and Christine Christensen present their abstract from the American Society of Pain and Neuroscience’s (ASPN) Third Annual Conference, where they discuss why the Streamlined Technique is a more minimally invasive procedural approach for the mild® Procedure and comparable to the Standard Approach in terms of its safety profile.
Eager to further understand the mild® Procedure and the technique described above? Contact Vertos Medical to learn more about the Streamlined Technique or check out the animation and physician experience from Dr. Jassal in this Procedure Evolution blog.
Navdeep Jassal, MD (00:01)
Hello, my name is Navdeep, Dr. Navdeep Jassal from the Spine Institute of Florida in Lakeland, Florida. I’m here to discuss a little bit about a study that is very meaningful to myself and especially my patients in my practice. We’re going to talk a little bit about the Streamlined Approach for the minimally invasive lumbar decompression or the mild® Procedure, and how that’s really changed the way I’ve practiced. We’re going to talk specifically about the safety profile for this particular technique and its comparison to the standard or the classical approach that we’ve used for years.
So what we did was we did a retrospective chart review on our patients and we just wanted to measure the incidence of postoperative complications of the Streamlined Technique compared to the Standard Approach. And we know that the Standard Approach is a very safe as well as an efficacious procedure, and we’ve seen this really time and time again, but classically we’ve seen this from the RCT from the MiDAS ENCORE study, which showed the approach of the Standard Approach, comparing the epidural steroid injection, which is the standard procedure that you do for patients with lumbar spinal stenosis with neurogenic claudication. And then comparing that with the mild® or the minimally invasive lumbar decompression procedure.
I wanted to take this a step further and I wanted to make sure that the complication rate was pretty much the same, which was extremely rare, comparing the Streamlined Approach with the Standard Approach and that’s simply what we did in this retrospective chart review in our practice. I’m going to turn it over to Christine Christensen, who is going to talk a little bit about the data and dive really further into the data because I think it’s just quite interesting.
Christine Christensen, MSN, APRN (02:06)
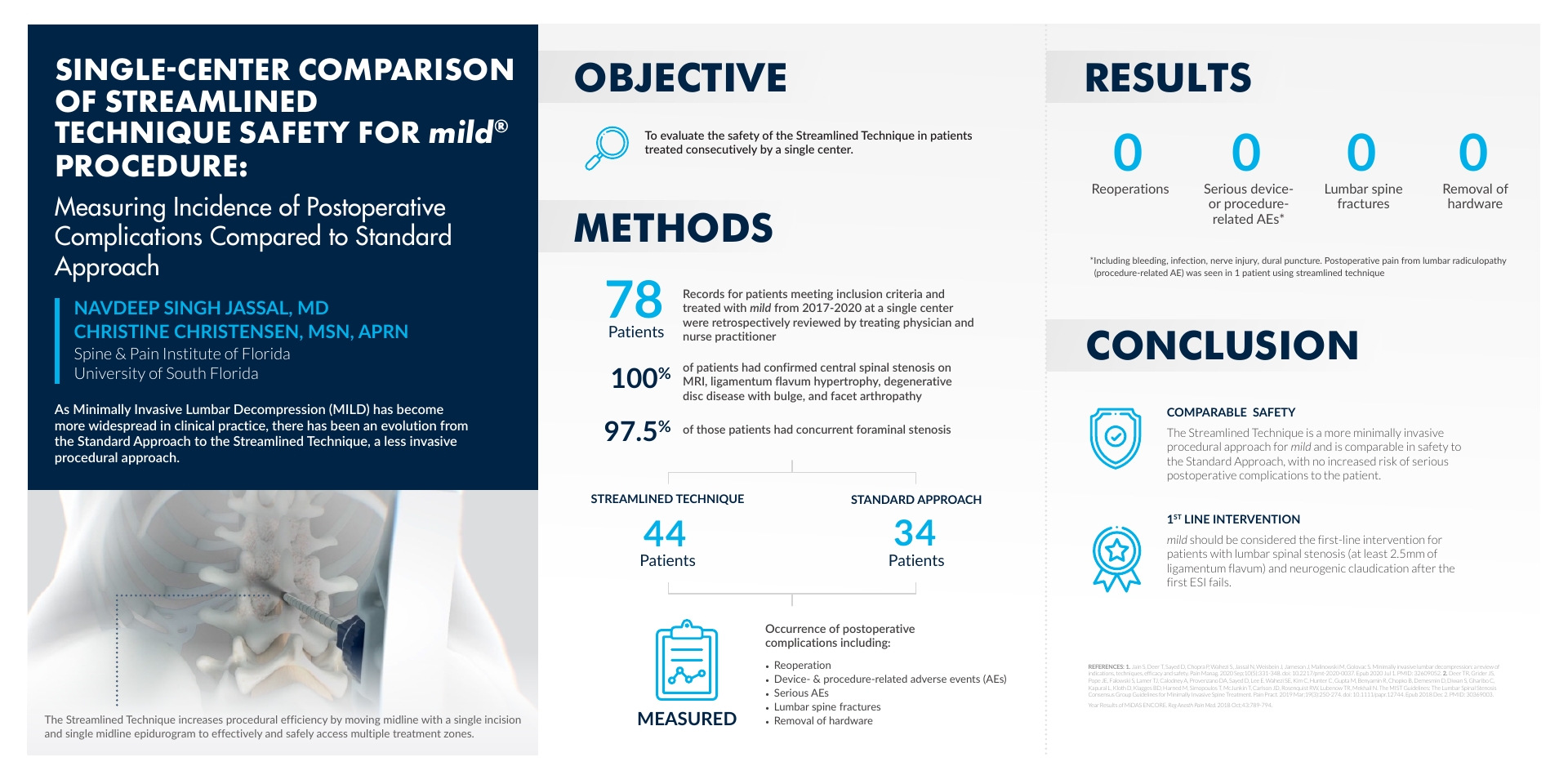
Hi, I’m Christine Christenson. I’m the Nurse Practitioner that works with Dr. Jassal here in Lakeland, Florida. As part of my practice here, Dr. Jassal was able to include me in generating data and analyzing that data for our research study here looking at the efficacy and safety of the Streamlined Technique. Now, data collection for this study consisted of reviewing charts on 78 patients that had the mild® Procedure performed for them. Dr. Jassal started doing the Streamlined Technique after certain dates.
So we looked at the date and the operative notes for those patients to verify that they did get the Streamlined Technique in the operating room. Of those patients, 100% had confirmed central spinal stenosis on MRI. They also had ligamentum flavum hypertrophy, degenerative disc disease with disc bulges, and facet arthropathy. Of the 78 patients, 97% had concurrent foraminal stenosis. So when we broke that down to the patients who had the Streamlined Technique after Dr. Jassal was trained in proper performance of the technique, we had 44 “streamlined” patients and then 34 patients who had the Standard Approach for the mild® Procedure.
So we took the 44 patients with the Streamlined Technique and the 34 Standard Approach patients and compared occurrence of postoperative complications, including reoperation, device- and procedure-related AEs, serious AEs, and lumbar spine fractures. We also did include removal of hardware, although we do know a big pro of the mild® Procedure is that there is no hardware placed into the patient, really maximizing patient benefit and minimizing risks for patients. This study did show that the Streamlined Technique did not have any increase in risk for patients versus the Standard Approach.
Navdeep Jassal, MD (04:13):
So in conclusion with our study, the Streamlined Technique is a more minimally invasive procedural approach for the mild® Procedure and it’s even comparable in terms of safety profile to the Standard Technique or the Standard Approach. There’s really no increased risk of serious postoperative complications to the patients. And we know that it’s comparable to the data that was shown in the ENCORE study or the RCT in the past.
Also, the mild® Procedure should be considered first-line intervention for patients with lumbar spinal stenosis, with neurogenic claudication symptoms, in a state where they know that they have at least 2.5 millimeters of ligamentum flavum on an MRI exam or a CAT scan study. So really they should be considered first-line intervention after conservative therapy is tried and even after the first epidural steroid injection is completed for your patient.
About Dr. Navdeep Jassal
 Navdeep Jassal, MD, is a Physiatrist and Interventional Pain Physician with a Fellowship in Pain Medicine from University of South Florida Morsani College of Medicine and board certifications in Pain Medicine and Physical Medicine and Rehabilitation. He completed a Residency in Physical Medicine and Rehabilitation at the Zucker School of Medicine at Hofstra/Northwell and received his Doctor of Medicine from Ross University School of Medicine. Dr. Jassal currently serves as an Assistant Professor for the Department of Physical Medicine & Rehabilitation at the University of Central Florida as well as an Assistant Clinical Professor for the University of South Florida’s Pain Medicine Fellowship program. Dr. Jassal is the Young Guys Co-chair for the American Society of Pain & Neuroscience (ASPN), Secretary for the Florida Society of Pain & Neuroscience (FSPN) and Section Editor for the Pain Physician Journal. He holds memberships with the American Society of Interventional Pain Physicians (ASIPP), Florida Medical Association (FMA), North American Neuromodulation Society (NANS), International Neuromodulation Society (INS), Florida Association of Physicians of Indian Origin (FAPI) and Association of Academic Physiatrists.
Navdeep Jassal, MD, is a Physiatrist and Interventional Pain Physician with a Fellowship in Pain Medicine from University of South Florida Morsani College of Medicine and board certifications in Pain Medicine and Physical Medicine and Rehabilitation. He completed a Residency in Physical Medicine and Rehabilitation at the Zucker School of Medicine at Hofstra/Northwell and received his Doctor of Medicine from Ross University School of Medicine. Dr. Jassal currently serves as an Assistant Professor for the Department of Physical Medicine & Rehabilitation at the University of Central Florida as well as an Assistant Clinical Professor for the University of South Florida’s Pain Medicine Fellowship program. Dr. Jassal is the Young Guys Co-chair for the American Society of Pain & Neuroscience (ASPN), Secretary for the Florida Society of Pain & Neuroscience (FSPN) and Section Editor for the Pain Physician Journal. He holds memberships with the American Society of Interventional Pain Physicians (ASIPP), Florida Medical Association (FMA), North American Neuromodulation Society (NANS), International Neuromodulation Society (INS), Florida Association of Physicians of Indian Origin (FAPI) and Association of Academic Physiatrists.
About Christine Christensen, MSN, APRN

Christine Christensen is a Nurse Practitioner who works as an Advance Practice Provider at the Spine & Pain Institute of Florida and partners closely with Dr. Navdeep Jassal. She completed her Bachelor of Science in Neuroscience at Brigham Young University. Christine then earned a Bachelor of Science in Nursing from the University of North Carolina at Chapel Hill and earned her Master of Science in Nursing at the University of Alabama at Birmingham.
The following study, “Evaluation of Safety and Efficacy of the Streamlined Technique vs the Standard Technique for Accessing Decompression Treatment Zones for the PILD Procedure,” investigates the safety and efficacy of the Streamlined Technique compared to the Standard Technique. While the PILD, or mild® Procedure, may be performed using both methods, the Streamlined Technique enables a single midline incision to access multiple treatment zones whereas the Standard Technique uses one incision per treatment zone. The study involved 243 patients that underwent the mild® Procedure using either technique and tracked their outcomes. The authors concluded that the Streamlined Technique does not compromise the safety or efficacy of the mild® Procedure. View the abstract poster below to learn why the Streamlined Technique is an innovative approach to consider.
Watch Dr. Dawood Sayed present his abstract from the American Society of Pain and Neuroscience’s (ASPN) Third Annual Conference, where he discusses how the study found that adopting the Streamlined Technique allowed for efficient and effective decompression of multiple treatment zones, without compromising the safety or efficacy of the mild® Procedure.
Eager to further understand the mild® Procedure and the technique described above? Contact Vertos Medical to learn more about the Streamlined Technique or check out the animation and physician experience from Dr. Navdeep Jassal in this Procedure Evolution blog.
Dawood Sayed, MD (00:00)
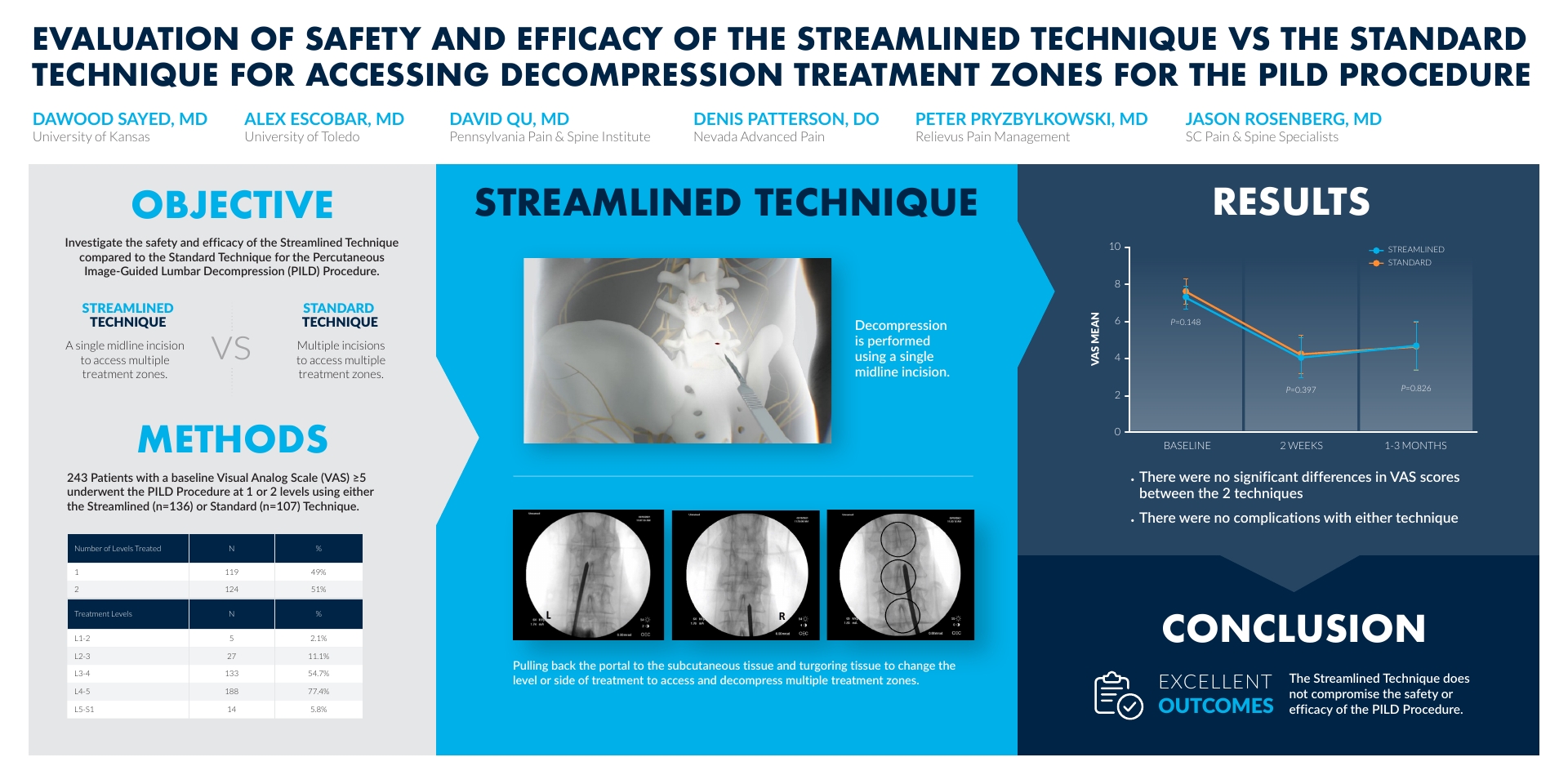
Hello, I’m Dr. Dawood Sayed and I’m a Professor of Anesthesiology and Pain Medicine at the University of Kansas. Today on behalf of my co-investigators, I’m gonna be presenting our abstract, an “Evaluation of the Safety and Efficacy of the Streamlined Technique vs the Standard Technique for Accessing Decompression Treatment Zones for the Percutaneous Interlaminar Lumbar Decompression (PILD) Procedure.” Our objectives were to investigate the safety and efficacy of the Streamlined Technique compared to the Standard Technique for the percutaneous image guided lumbar decompressive procedure. In summary, the Streamlined Technique is a single midline incision to access multiple treatment zones versus the more traditional standard techniques, in which multiple incisions are made to access multiple treatments zones. It was the hypothesis of the investigators, that using the Streamlined Technique, that we would be able to perform the procedure in an equal satisfactory manner with the same efficacy, but also performing the procedure in a much less invasive manner for the patient.
(01:03) So our methods were 243 patients with a baseline visual analog score of greater than five. These patients underwent the PILD Procedure at 1 or 2 treatment levels using either the Streamlined Technique which is about 136 patients, or the Standard Technique, which was about 107 patients. If you look at the table here, you can see that most of the patients were treated at either the L-3, L-4 or the L-4, L-5 levels. And again, the Streamlined Technique is a decompression performed using a single midline incision. The technique involves pulling back the portal to the subcutaneous tissue, and triggering tissue to change the level or side of treatment, to access and decompress multiple treatment zones through a single incision. When we look at our results, you can see the average pain level was around an 8 on a VAS mean score. When you look at the immediate pain relief and efficacy at around 2 weeks, you can see that the difference between the results and efficacy between the Standard Technique and the Streamlined Technique was almost identical. When you look at these patients a little further out at 1 to 3 months, again, you can see no difference in the outcomes in pain scores, as well as complication rates between the two arms when comparing the Streamlined and Standard Technique. So in conclusion, the Streamlined Technique does not compromise safety or efficacy of the PILD Procedure. We look forward to evaluating this in a more prospective, rigorous manner, to evaluate it as a true change in the way we do this procedure. Thank you.
Most Minimally Invasive Lumbar Decompression (mild®) providers are very familiar with the 1-year study conducted by Nagy Mekhail, MD, PhD who, along with a team of investigators from the Department of Pain Management at the Cleveland Clinic, examined the real-world benefit of the mild® Procedure: functional improvement. The 1-year outcomes demonstrated significant functional improvement for lumbar spinal stenosis (LSS) patients in both walking distance and standing time, with continuous mean improvement at each follow-up point. The study results are remarkable, as can be viewed in the figure below.

Patients clearly benefited from this type of treatment with a notable increase in function; this shows the effect the mild® Procedure had on patients who were previously unable to complete simple, everyday tasks beforehand. Now they are able to get out and enjoy life without having to sit down and rest as frequently as they did before the mild® Procedure.
The investigators at the Cleveland Clinic recently published an additional independent, retrospective cohort study which further explores the long-term durability of mild® at 5 years. They followed LSS patients receiving the mild® Procedure at the Cleveland Clinic between 2010 and 2015.
The recently published paper, The Durability of Minimally Invasive Lumbar Decompression Procedure in Patients with Symptomatic Lumbar Spinal Stenosis: Long Term Follow-Up, explores how many patients were able to avoid surgical decompression after the mild® Procedure over a five-year period. Changes in pain level using the Numeric Rating Scale (NRS) and opioid medication utilization using Morphine Milligram Equivalent (MME) dose per day from baseline to 3-, 6-, and 12-months post-mild® Procedure were also collected, along with post-procedure complications.
mild® is a minimally invasive decompression procedure that addresses a major root cause of patients’ stenosis without having to undergo an invasive open surgery or leave implants behind. It has the safety profile equivalent to an epidural steroid injection (ESI), but with lasting results and is often compatible for patients with existing risk factors that, traditionally, may not be candidates for open surgery. According to the study, the mild® Procedure significantly decreased the incidence of surgical decompression at the same treatment level(s) as mild® intervention during five-year follow-up. Nine out of 75 patients required lumbar surgical decompression at the same level during the follow-up period, making the annual incidence of same-level lumbar-decompression surgery just 2.4%. Subjects experienced statistically significant pain relief and reduction of opioid medications utilization at 3, 6, and 12 months compared to baseline. There were no major complications reported.
Here are the 3 key takeaways from the 5-year study, and a link to access the full peer-reviewed articles:

88% of patients avoided surgical decompression for at least 5 years.
“The durability of mild® over 5 years may allow elderly patients with symptomatic lumbar spinal stenosis to avoid lumbar decompression surgery while providing significant symptomatic relief.”

No implants.
“The mild® Procedure allows debulking of the hypertrophic ligamentum flavum without interfering with the integrity of the bony spine, and does not require implants.”

No need to delay patient care.
“Further, because the mild® procedure demonstrated durability up to 5 years, it might also be speculated with caution, that appropriate patients should be encouraged to undergo the mild® procedure as early as needed, rather than waiting until these patients are at an advanced age.”
View 5-Year Paper View 1-Year Paper
Acknowledgments: A special thank you to the investigator and author team from the Evidence-Based Pain Management Research Group at the Cleveland Clinic: Nagy Mekhail, MD, PhD; Shrif Costandi, MD; George Nageeb, BS; Catherine Ekladios, MD; Ogena Saied, MS. Vertos Medical and the mild® patients across the country who benefit from this procedure are grateful for your care and attention in advancing the data around the safety, functional improvement, and long-term durability of mild®.
Benyamin RM, Staats PS, MiDAS ENCORE Investigators. mild® is an effective treatment for lumbar spinal stenosis with neurogenic claudication: MiDAS ENCORE Randomized Controlled Trial. Pain Physician. 2016;19(4):229-242.
Mekhail N, Costandi S, Abraham B, Samuel SW. Functional and patient-reported outcomes in symptomatic lumbar spinal stenosis following percutaneous decompression. Pain Pract. 2012;12(6):417-425. doi:10.1111/j.1533-2500.2012.00565.x.
2012 data from Health Market Sciences report for Vertos Medical 2013.
Data on file with Vertos Medical.
Staats PS, Chafin TB, Golvac S, et al. Long-term safety and efficacy of minimally invasive lumbar decompression procedure for the treatment of lumbar spinal stenosis with neurogenic claudication: 2-year results of MiDAS ENCORE. Reg Anesth Pain Med. 2018;43:789-794. doi:10.1097/AAP.0000000000000868.
Based on mild® Procedure data collected in all clinical studies. Major complications are defined as dural tear and blood loss requiring transfusion.
MiDAS ENCORE responder data. On file with Vertos Medical.
Jain S, Deer TR, Sayed D, et al. Minimally invasive lumbar decompression: a review of indications, techniques, efficacy and safety. Pain Manag. 2020;10(5). https://doi.org/10.2217/pmt-2020-0037. Accessed June 1, 2020.
Deer TR, Grider JS, Pope JE, et al. The MIST Guidelines: the Lumbar Spinal Stenosis Consensus Group guidelines for minimally invasive spine treatment. Pain Pract. 2019;19(3)250-274. doi:10.1111/papr.12744.
Hansson T, Suzuki N, Hebelka H, Gaulitz A. The narrowing of the lumbar spinal canal during loaded MRI: the effects of the disc and ligamentum flavum. Eur Spine J. 2009;18(5):679-686. doi:10.1007/s00586-009-0919-7.
Treatment options shown are commonly offered once conservative therapies (e.g., physical therapy, pain medications, chiropractic) are not providing adequate relief. This is not intended to be a complete list of all treatments available. Doctors typically recommend treatments based on their safety profile, typically prioritizing low risk/less aggressive procedures before higher risk/more aggressive procedures, but will determine which treatments are appropriate for their patients.
The mild® Procedure is a minimally invasive treatment for lumbar spinal stenosis. As with most surgical procedures, serious adverse events, some of which can be fatal, can occur, including heart attack, cardiac arrest (heart stops beating), stroke, and embolism (blood or fat that migrates to the lungs or heart). Other risks include infection and bleeding, spinal cord and nerve injury that can, in rare instances, cause paralysis. This procedure is not for everyone. Physicians should discuss potential risks with patients. For complete information regarding indications for use, warnings, precautions, and methods of use, please reference the devices’ Instructions for Use.
Patient stories on this website reflect the results experienced by individuals who have undergone the mild® Procedure. Patients are not compensated for their testimonial. The mild® Procedure is intended to treat lumbar spinal stenosis (LSS) caused by ligamentum flavum hypertrophy. Although patients may experience relief from the procedure, individual results may vary. Individuals may have symptoms persist or evolve or other conditions that require ongoing medication or additional treatments. Please consult with your doctor to determine if this procedure is right for you.
Reimbursement, especially coding, is dynamic and changes every year. Laws and regulations involving reimbursement are also complex and change frequently. Providers are responsible for determining medical necessity and reporting the codes that accurately describe the work that is done and the products and procedures that are furnished to patients. For this reason, Vertos Medical strongly recommends that you consult with your payers, your specialty society, or the AMA CPT regarding coding, coverage and payment.
Vertos Medical cannot guarantee coding, coverage, or payment for products or procedures. View our Billing Guide.
Vertos is an equal employment opportunity workplace committed to pursuing and hiring a diverse workforce. We strive to grow our team with highly skilled people who share our culture and values. All qualified applicants will receive consideration for employment without regard to sex, age, color, race, religion, marital status, national origin, ancestry, sexual orientation, gender identity, physical & mental disability, medical condition, genetic information, veteran status, or any other basis protected by federal, state or local law.
Hall S, Bartleson JD, Onofrio BM, Baker HL Jr, Okazaki H, O’Duffy JD. Lumbar spinal stenosis. Clinical features, diagnostic procedures, and results of surgical treatment in 68 patients. Ann Intern Med. 1985;103(2):271-275. doi:10.7326/0003-4819-103-2-271.
Kalichman L, Cole R, Kim DH, et al. Spinal stenosis prevalence & association with symptoms: The Framingham Study. Spine J. 2009;9(7):545-550. doi:10.1016/j.spinee.2009.03.005.
Fukusaki M, Kobayashi I, Hara T, Sumikawa K. Symptoms of spinal stenosis do not improve after epidural steroid injection. Clin J Pain. 1998;14(2):148-151. doi:10.1097/00002508-199806000-00010.
Mekhail N, Costandi S, Nageeb G, Ekladios C, Saied O. The durability of minimally invasive lumbar decompression procedure in patients with symptomatic lumbar spinal stenosis: Long-term follow-up [published online ahead of print, 2021 May 4]. Pain Pract. 2021;10.1111/papr.13020. doi:10.1111/papr.13020
Friedly JL, Comstock BA, Turner JA, et al. Long-Term Effects of Repeated Injections of Local Anesthetic With or Without Corticosteroid for Lumbar Spinal Stenosis: A Randomized Trial. Arch Phys Med Rehabil. 2017;98(8):1499-1507.e2. doi:10.1016/j.apmr.2017.02.029
Pope J, Deer TR, Falowski SM. A retrospective, single-center, quantitative analysis of adverse events in patients undergoing spinal stenosis with neurogenic claudication using a novel percutaneous direct lumbar decompression strategy. J Pain Res. 2021;14:1909-1913. doi: 10.2147/JPR.S304997
Pryzbylkowski P, Bux A, Chandwani K, et al. Minimally invasive direct decompression for lumbar spinal stenosis: impact of multiple prior epidural steroid injections [published online ahead of print, 2021 Aug 4]. Pain Manag. 2021;10.2217/pmt-2021-0056. doi:10.2217/pmt-2021-0056
Abstract presented at: American Society of Pain and Neuroscience Annual Conference; July 22-25, 2021; Miami Beach, FL.
Mobility Matters: Low Back Pain in America, Harris Poll Survey, 2022. View data and full summary here.
Deer TR, Grider JS, Pope JE, et al. Best Practices for Minimally Invasive Lumbar Spinal Stenosis Treatment 2.0 (MIST): Consensus Guidance from the American Society of Pain and Neuroscience (ASPN). J Pain Res. 2022;15:1325-1354. Published 2022 May 5. doi:10.2147/JPR.S355285.